
{kind=link}
Ever since antivaccine and pharma conspiracy theorist and enemy of public health Robert F. Kennedy, Jr. suspended his quixotic campaign for the Presidency to bend the knee to Donald Trump, in return for the promise of a high-ranking position in Trump’s administration related to health policy—and especially since Donald Trump won the election two weeks ago—I’ve been writing about what a horror he could be for public health, regardless of the position to which he ended up being appointed. Then, over a week ago, we learned that President-Elect Trump plans to appoint him as Secretary of the Department of Health and Human Services, something that I had been speculating as a strong possibility and likely the worst-case scenario, given that the HHS Secretary is in charge of basically all non-military medical and health policy and oversees the critical health infrastructure in the department, which includes the Centers for Disease Control and Prevention (CDC), the Food and Drug Administration (FDA), the National Institutes of Health (NIH), and the Centers for Medicare and Medicaid Services (CMS). Truly, RFK Jr., if confirmed by the Senate—which he might well be even in spite of his antivax conspiracy-mongering and stories about his having had a brain worm, dumped a road-kill bear cub in Central Park ten years ago, and decapitated a dead whale to take the head home—will be a catastrophe for federal health policy and medical research. (Sadly, the only thing that I see maybe tripping up his confirmation is his past strong support for abortion rights.)
Given his antivaccine background, burbling from the Trump campaign that RFK Jr. wanted access to federal vaccine safety databases in order to “prove” vaccines are unsafe as a pretext for taking them off the market, and his threat to “declare war” on the FDA, at first I concentrated mainly on the FDA and the Centers for Disease Control and Prevention, in particular the damage that he might do to the CDC’s vaccination program, but equally important is what he might do to the National Institutes of Health, arguably the greatest engine of biomedical research ever created. When I saw news stories floating around this weekend that high on the list of candidates for NIH Director is a name familiar to our readers, namely Dr. Jay Bhattacharya, coauthor of the Great Barrington Declaration, that famous anti-public health manifesto calling for a “let ‘er rip” approach to the pandemic—in October 2020, before there was a vaccine!—with the futile goal of achieving “natural herd immunity,” with a poorly defined strategy of “focused protection” that would supposedly keep those most vulnerable to severe disease and death from COVID-19 while the presumably young and healthy died at a much lower rate than the elderly and ill as the virus rampaged through the population. It was a tendentiously libertarian and profoundly social Darwinist approach to “open up the economy” at the expense of disease and death that never would have worked and ultimately caused enormous damage to public health.
[Update: It’s official. Dr. Bhattacharya is the nominee to run NIH.]
I knew when I saw these stories that I had to discuss the consequences to the NIH of having an antivax conspiracy theorist who wants to devote half of NIH resources to “chronic diseases” in charge of the department under which NIH falls and a director likely handpicked by him. Spoiler alert: It won’t be good. At all.
How the NIH doles out money
Over 80% of NIH funding goes to funding extramural research grants (extramural=not funding labs at the NIH itself). Contrary to the conspiracist vision of Anthony Fauci—or any other Institute director at NIH, or even the NIH director him or herself —personally viewing every grant application and deciding who gets those sweet, sweet NIH dollars and who does not, there is a long-defined, rigorous, and codified process used by the NIH to evaluate grants applications. It begins with the submission of a grant to the NIH. Before I discuss what happens next, I will note that the NIH has a number of granting mechanisms designed for different purposes. For example, the R21 grant is designed for preliminary work, often the “higher risk” studies that the brave mavericks demand, and doesn’t require a lot of preliminary data. (The claim that it can require no preliminary data, however, is generally nonsense. You need at least some data.) R21s can fund up to two years and cannot be renewed.
In contrast, the granddaddy of them all, the “gold standard” grant for an individual investigator, small groups of co-investigators, or collaborators, is the R01, which can be funded for up to five years (it’s also one of the only grant mechanisms where the investigator can propose basically anything, rather than having to address a particular topic or question). At the end of that time, the investigator can apply for a competitive renewal, which can extend the grant for up to another five years, and so on ad infinitum. There are a number of other grant mechanisms, which include training grants for graduate students, center grants (e.g., for cancer centers), larger multi-investigator grants, and more targeted grants—Wikipedia has a nice list here—but in general all of them are scored by groups of scientists with the relevant expertise in a review group called a study section, of which there are dozens in the NIH arranged by topic into Review Branches at the Center for Scientific Review. Many of these study sections are permanent, but the NIH can and does set up temporary study sections for topics of special interest at the time.
NIH grants generally undergo two levels of review, first the study section and then advisory councils. To guide the reviews, the NIH has five criteria that it uses to evaluate grant applications:
- Significance
- Investigator(s)
- Innovation
- Approach
- Environment
Other considerations include “Additional Review Criteria”:
As applicable for the project proposed, reviewers will evaluate the following additional items while determining scientific and technical merit and in providing an overall impact score, but will not give separate scores for these items.
- Study Timeline (specific to applications involving clinical trials)
- Protections for Human Subjects
- Inclusion of Women, Minorities, and Children
- Vertebrate Animals
- Biohazards
- Resubmission
- Renewal
- Revision
Additional Review Considerations. As applicable for the project proposed, reviewers will consider each of the following items, but will not give scores for these items and should not consider them in providing an overall impact score.
- Applications from Foreign Organizations
- Select Agent
- Resource Sharing Plans
- Authentication of Key Biological and/or Chemical Resources
- Budget and Period Support
Grants undergo anonymous peer review, and usually each application is reviewed by three or four reviewers, with one of them being a statistician where appropriate. Those assigned to do the detailed reviews score each of the above areas from 1-9, although in this case low scores are better, denoting high impact/priority, and then assign an overall impact score to the grant application. During the study section meeting, the study section member assigned as primary reviewer starts the discussion with a summary of the grant application, the score assigned to it, and why that score was assigned. Then the others who evaluated each grant application do the same, after which the whole study section discusses the application. At the end, every member assigns an overall impact score to the grant under discussion before moving on to the next application. After the study section meeting, all the impact scores are used to calculate a final overall Priority Score assigned to the grant application. Also, the membership rosters of the study sections are public knowledge, as they are published on the CSR website; so it’s not uncommon for investigators who got a bad review among their reviews to make a good guess about who was responsible.
Although I’ve never served as a permanent member of an NIH study section, I have served as an ad hoc member for specific expertise. (Ad hoc members generally serve for only one or a handful of grant review cycles, rather than being assigned for multi-year stints.) As such, I can only comment on the dynamics of study sections in which I’ve participated. One thing that I’ve noticed is that it only takes one highly negative review from a reviewer who is outspoken to tank an application. I’ve also noted that someone who really likes a grant application can sway others to score it higher, but the effect seems a bit weaker than “negative campaigning,” which seems more effective in getting others to lower their scores.
When an individual grant application hits the NIH, it will be assigned to a study section. Investigators can influence this process by suggesting study sections, and, unsurprisingly, some study sections have reputations for being harsher than others. Once a grant is assigned to a study section, that study section’s Scientific Review Officer (SRO) will read it, decide if it’s appropriate for the study section, and assign reviewers:
Assignment of Applications to Specific Reviewers: The SRO assigns applications to particular reviewers by matching the science in the application to the reviewer’s expertise. Assignment considerations include: reviewer knowledge about, and interest in, the goals of the project; expertise in the techniques proposed; reviewer workload; and real or perceived conflicts of interest. The SRO encourages reviewers to let him/her know of any concerns that they have about their assignments. This would include conflicts of interest, concerns about the appropriateness of the assignment, or the need for additional expertise.
The SRO also recruits scientists to serve on the study section, thusly:
Identifying and Recruiting Reviewers: Possibly the most important role of the SRO is to ensure that the reviewers present at the study section meeting have all the needed expertise to evaluate the applications under review.
In choosing regular members for study sections, it is essential that the SRO recognizes current trends in the field and ensures that the membership reflects where the field is now and where it is going. It is also critical that the expertise of each nominee complements that of the other members and strengthens the study section as a whole.
As you can see, the SRO is a big deal.
The SRO also runs the study section meeting, collates the reviews, takes notes, and from those notes and the overall reviews produces a Summary Statement that includes the overall Priority Score assigned (with a percentile measurement denoting the percentage of grant applications that were scored higher than the applicant’s), comments about the discussion at the study section, and the original “raw” reviews from each study section member who reviewed the grant. Note that now generally only grants that score in the top one-third to one-half receive overall Priority Scores and Summary Statements, because any grant with higher (and therefore worse) scores are so unlikely to be funded as to make it not worth the SRO’s effort to put the documents together. These investigators do, however, still receive the reviews carried out by individual study section members. SROs also handle appeals from applicants who question whether their review was fair or whether one or more of the reviewers had the requisite expertise.
The second level of review occurs through committees formed at each Institute and Center (IC) at the NIH called Advisory Councils:
The Advisory Council/Board of the potential awarding Institute/Center performs the second level of review (See Advisory Councils or Boards). Advisory Councils/Boards are composed of scientists from the extramural research community and public representatives (NIH Federal Advisory Committee Information). Members are chosen by the respective IC and are approved by the Department of Health and Human Services. For certain committees, members are appointed by the President of the United States.
Now here’s the part where the conspiracy might come in:
Recommendation Process
- NIH program staff members examine applications and consider the overall impact scores given during the peer review process, percentile rankings (if applicable) and the summary statements in light of the Institute/Center’s priorities.
- Program staff provide a grant-funding plan to the Advisory Board/Council. Council members have access to applications and summary statements pending funding for that IC in that council round.
- Council members conduct a Special Council Review of grant applications from investigators who currently receive $1 million or more in direct costs of NIH funding to support Research Project Grants (see NOT-OD-12-140). This additional review is to determine if additional funds should be provided to already well-supported investigators and does not represent a cap on NIH funding.
- The Advisory Council/Board also considers the Institute/Center’s goals and needs and advises the Institute/Center director concerning funding decisions.
- The Institute/Center director makes final funding decisions based on staff and Advisory Council/Board advice
It’s that last part that the conspiracy theorists harp on. In theory, an Institute director like Anthony Fauci could override all the peer review to fund a grant, but in practice it almost never happens. Why? Because the NIH set up this process in order to minimize the possibility direct involvement of its leaders in picking and choosing grant awardees based on personal whim. The whole system exists to try to ensure as much as possible that grant selection is based on scientific merit, and few other considerations.
I won’t go through the whole appeals process, other than to say that appeals rarely succeed. I also won’t say that politics and the personal preferences of various Institute/Center (IC) directors never play a role in grant funding decisions, but I will say that the system is set up to minimize such biases playing a significant role in funding decisions. Also, often the people who most characterize NIH funding decisions as the personal doling out of funding by directors are the same ones who have no compunction about trying to shut down research they don’t like themselves—and have been for a long time.
Add to this efforts by the NIH to minimize repetitional bias, in which, all things being equal, more highly ranked universities and researchers are more likely to be funded than researchers with a lower reputation or at a university with a lower reputation, and the system is complex, full of safeguards, and designed to work as close to a meritocracy as possible. It is imperfect, of course, and often doesn’t achieve that goal, but reforming the system so that it comes closer is clearly not what RFK Jr. is about, given that he’s described big pharma as a “criminal enterprise,” with the NIH, FDA, and CDC all in cahoots with it.
RFK Jr.’s plans for NIH
Before I get to discussing why Jay Bhattarcharya (or, likely, any nominee that RFK Jr. could propose and persuade President-Elect Trump to agree to) would be such a dumpster fire as NIH Director, let’s take a look at what RFK Jr. has been saying about NIH and his plans for it. Last week, for instance, RFK Jr. was quoted as saying:
At an event late last week in Arizona, anti-vaccine activist and Donald Trump transition team member Robert F. Kennedy Jr. said he’d fire and replace 600 people from the National Institutes of Health on day one of a second Trump term. The NIH is one of the public health agencies Kennedy loathes the most—and despite still lacking any defined role in a new administration, he’s clearly relishing the opportunity to promise retribution against them.
In comments that were first reported by ABC News, Kennedy declared, “We need to act fast, and we want to have those people in place on January 20, so that on January 21, 600 people are going to walk into offices at NIH and 600 people are going to leave.”
Of course, RFK Jr. loathes the NIH. Besides its having been the longtime employer of his nemesis Dr. Anthony Fauci, who ran the National Institute of Allergy and Infectious Diseases from the 1980s until his recent retirement, one key strength of the NIH over its entire existence has been its general independence from partisan politics and focus on the best science and medicine, which automatically excludes RFK Jr. No one is saying NIH is perfect, certainly not I, but it is about as close as one can get to a genuine scientific meritocracy in a federal agency as one can imagine. Moreover, whatever complaints one might have about its system for determining which research grant applications receive funding as being too “safe” or conservative, complaints resurrected by COVID-19 contrarians during the pandemic, it does try to adhere to a very rigorous process of scientific peer review by its study sections to score grants and rank them for funding priority. Could the process be improved to be made fairer, more rigorous, and more open to less “safe” ideas? Yes. Does RFK Jr. have clue one how to do that? No. It’s not even what he’s about, which is to direct some of that sweet, sweet NIH grant money to his antivax quack cronies, whom he views as having been unjustifiably “silenced.”
What RFK Jr. seems to be proposing here is to replace directors, managers, and scientists whom he doesn’t like with political loyalists. This statement is also yet more evidence that he doesn’t have clue one how NIH operates. There are only around 200 political appointees in the entire HHS and just a handful at NIH. At the NIH, most employees are the scientists and physicians who do biomedical research and oversee the review process for deciding which grant applications are funded, as well as the support staff to assist them and to administer yearly grant allocations and the reporting requirements for those receiving NIH grants. Again, the NIH has long been one of the most apolitical and nonpartisan agencies in the entire federal government, which has been its traditional strength. Moreover, there is a culture there that very much resists attempts by legislators and politicians to influence its scientific decisions, even at the National Center for Complementary and Integrative Health, which does research most aligned with RFK Jr.’s stated priorities.
Given Kennedy’s history, you know that his picks will all be hacks, quacks, and conspiracy theorists. It is also not at all clear that he can do this, given federal civil service protections. It is clear how he wants to realign research priorities at the NIH as well:
Calley Means, a self-described health care reform activist who played a role in Kennedy’s independent presidential run sat alongside him for part of the interview. He framed the MAHA movement as “kicking the special interests and the Deep State” out of government, calling the NIH “an orgy of corruption.”
Kennedy made other eyebrow-raising claims during the interview, for instance claiming that “pilot studies” showed that anorexia could be cured with a “keto diets and other kind of diets.”
“NIH won’t do those studies because they don’t want to know the source or the cure or the treatment of chronic disease,” he declared. He also returned to his hobby horse, claiming links between vaccines and a spread in autism.
“I never saw anybody who was autistic when I was a kid,” Kennedy claimed. “Never.” He added that men his age—Kennedy is 70—don’t have “full blown autism,” which he defined as “wearing helmets” and “not being toilet trained” and “head-banging, stimming, toe-walking.”
We’ve written about the brother-sister duo of Calley and Casey Means before. Casey Means is a former otolaryngology resident who quit in her last year of residency to peddle “alternative health,” while her brother runs a business that facilitates people using health savings accounts to purchase quackery. No one should be surprised at anything that Kennedy said here. It’s just RFK Jr. being RFK Jr., the same nonsense that he’s been spewing at least since 2005 about vaccines causing autism. As always, he continues to confuse correlation with causation and blame vaccines for a phenomenon that reflects far more on broadening of the diagnostic criteria for autism spectrum disorders in the 1990s, increased screening and surveillance, and a better understanding of the underlying neurodevelopmental contributors to autism than any biological basis for an increase in measured prevalence.
RFK Jr. vs. “conflicts of interest”?
A couple of months ago, not long after he had bent the knee to Donald Trump, RFK Jr. published an op-ed in The Wall Street Journal entitled entitled Trump Can Make America Healthy Again, which was subtitled, “Chronic diseases have reached crisis proportions, and Kamala Harris seems uninterested in the issue.” In it, RFK Jr. laid out a 12-point plan to “make America healthy again,” which spawned MAHA, to go along with MAGA (“make America great again”). I discussed his plan in depth then, noting how assiduously RFK Jr. hid his antivax proclivities given that vaccines weren’t mentioned even once in the plan (something his antivax supporters noticed immediately and did not like). Suffice to say that the plan was a lot of the same ol’ same ol’ about supposed corruption at the FDA; his old claim, at best highly dubious and exaggerated and at worst false, that children today represent America’s “sickest generation” (and a lot of it is due to—cough, cough—vaccines); rants about pesticides; and the usual pharma conspiracy mongering. While it is true that one part of his proposal, finding ways to decrease conflicts of interest among scientists and doctors tasked with regulating health, was fairly mainstream, the devil is in the details, and we all know that RFK Jr.’s definition of a “conflict of interest” is very different from the standard definition; at the very least he has a double standard, identifying involvement with pharma as a COI but ignoring massive COIs among his favored quacks, most of whom make their living selling nostrums, quackery, and supplements.
Let’s revisit, however, what RFK Jr. wrote in his September WSJ op-ed describing what he wanted to do with the NIH, first:
Change federal regulation so that NIH funds can’t go to researchers with conflicts of interest. A 2019 ProPublica analysis of disclosures going back to 2012 found that over 8,000 federally funded health researchers reported significant financial conflicts of interest.
I asked at the time: According to RFK Jr.’s definition, what constitutes a “conflict of interest” for an NIH-funded researcher? Once again, I remind our readers that many of these researchers are trying to translate their findings into actual medical products that benefit patients, be they new drugs, devices, or other treatments designed to prevent and treat specific diseases. To do so, they often either form companies themselves or partner with existing companies to continue to develop their findings from the basic science and preclinical stages into an FDA-approvable, marketable product ready to undergo randomized clinical trials for FDA approval. There are even NIH grant mechanisms specifically designed to assist this process, like the Small Business Innovation Research (SBIR) and Small Business Technology Transfer (STTR) programs, collectively the Small Business Programs, also known as America’s Seed Fund.
Last year, during an interview with Lex Fridman, RFK Jr. pontificated about what he meant when it came to NIH “COIs”:
From around the 7:00 mark:
In fact there’s a word for those kind of scientists who take money for their opinion and the words by biostitutes and they are very very common and you know and I’ve been dealing them with, with them my whole career. You know, I think it was Upton Sinclair who said that it’s very difficult to persuade a man of a fact if the existence of that fact will diminish his salary and I think that’s true for all of uf. If they, you know, we find a way of reconciling ourselves the things that are the truth that actually and world wiews and actually benefit our our salaries.
Now NIH, um, NIH has probably the worst system which is that scientists who work for NIH—NIH itself which used to be the premier gold standard scientific agency in the world. Everybody looked at NIH. Today it’s just an incubator for pharmaceutical drugs, and, and, you know, that is that gravity of economic self-interest because if you’re, um, if NIH itself collects uh royalties, they have margin rights for the patents, on all the drugs that they work on. So, with the Moderna vaccine which they, promoted incessantly and NIH on 50% that vaccine is making billions and billions of dollars on it, and there are four at least four scientists that we know of and probably at least six at NIH who themselves have margin rights for those patents. So if you are a scientist who work at NIH you work on a new drug you you then get margin rights and you’re entitled to royalties 150,000 a year forever from that forever—your children, your children’s children. As long as that, uh, product’s on the market you can collect royalties. So you have you know the modern vaccine is paying for the top people at NIH, you know some of the top regulators is paying for their boats it’s paying for their mortgages paying for their children’s education and you know you have to expect that the uh that in those kind of situations the regulatory function would be um subsumed beneath the mercantile ambitions of the agency itself and the individuals who stand to profit enormously from getting a drug to market. Those guys are paid by us the taxpayer to find problems with those drugs before they get to Market but if you know that drug is going to pay for your mortgage you may overlook a little problem and that we’re even a very big one and that’s the problem.
A couple of points in response: First, I hate the term “biostitute.” It’s a term that RFK Jr. has long used to describe scientists and physicians whom I admire for their pro-vaccine and pro-science advocacy, especially Dr. Paul Offit. Second, and more importantly, what planet is RFK Jr. living on? His description of how things work bears little resemblance to how things actually work with respect to royalties to the NIH from pharmaceutical companies who use NIH-funded research to develop marketable products. One of the better debunking of this conspiracy theory was published this June in Science, in response to its being claimed by Rep. Marjorie Taylor Greene, who claimed that the NIH had pocketed $710 million in royalties from COVID-19 vaccines and that Fauci had personally collected millions.
In reality:
A series of laws passed by Congress starting in the 1980s that aimed to spur innovation and sharing of technology allows federal employees to receive a limited share of the royalties. But NIH scientists can legally only earn up to $150,000 a year in royalties, which Andrzejewski tells Science
Insider he knew, although it wasn’t disclosed in his article. And the reality that almost all of the $710 million went back to the U.S. government is also easy to verify on a long-standing, public NIH website about royalty distributions from technology transfers.*In one exchange with Fauci, Malliotakis asked whether he thought that “any of those royalties, this nearly billions [sic] of dollars, should be going back to the American taxpayer, not in the pockets of the scientists?”
In fact, NIH said most of the royalty income that comes to institutes and centers “supports additional research,” noting that U.S. law stipulates how it may be used, including a requirement that money be given to the U.S. Department of the Treasury if the amount exceeds 5% of an agency’s annual budget.
It is true that the NIH does not routinely disclose how much in royalties individual scientists receive. If all RFK Jr. wanted to do was something like the the Royalty Transparency Act, a bill with broad bipartisan support that would require the NIH to disclose this information, I could be on board with that. However, somehow I doubt that’s what he has in mind, given that he is lying about the situation. Yes, I say “lying,” because as a lawyer RFK Jr. knows all the information cited above and that how royalties to the NIH from pharmaceutical companies using its research are distributed is mandated by law. Indeed, he must know that the vast majority of the payments in the report commonly cited by cranks like RFK Jr. predate the pandemic.
Also:
Fauci’s payments came from Santa Cruz Biotechnology, a company that develops products for biomedical research. Santa Cruz Biotechnology made 13 other payments to Fauci from 2010 to 2019.
When the Associated Press wrote in 2005 about previous royalties paid to Fauci, and how the payments raised concerns about potential conflicts of interest, Fauci said he planned to donate all royalties that he receives to charity. He told the AP that he tried to refuse the royalties, but was told that he was legally obligated to accept the money.
Again, one can argue that the royalty payments mandated by law for the last few decades are a problem. One can argue that perhaps they should be curtailed or at least more fully disclosed, but consider this. RFK Jr. is also lying about the NIH. The NIH has no regulatory function when it comes to drug approval; its scientists are not taking royalties from pharmaceutical companies whose products they are approving. RFK Jr. knows that, but he also knows that most Americans don’t know that. So he lies.
No one, least of all I, will argue that COIs shouldn’t be reported. Moreover, the NIH does require its investigators to report any financial COI that involves more than $5,000/year. (I know this because as faculty at a university that receives NIH funding, every couple of years I have to do online training about COIs). If the goal of NIH-funded research is to lay the groundwork for drugs, treatments, and devices that are ultimately turned into products it is counterproductive to ban NIH funds from going to anyone who has a financial interest with a pharmaceutical, medical device, or food company. One can reasonably argue about policies designed to minimize harmful influences due to financial COIs and how to make sure that all COIs are reported and findable by the public, but to ban researchers with interest in a company related to the research that they are carrying out would likely have the unintended consequence of seriously hampering further research. The issue is, of course, complex, predictably RFK Jr. has presented an oversimplified version of it designed to imply that most NIH researchers are in the pocket of big pharma, all as a pretext towards, likely, undertaking a witch hunt for scientists with COIs that he thinks he can fire.
The NIH and chronic disease
Next up, from RFK Jr.’s MAHA manifesto published in the WSJ:
Devote half of research budgets from the NIH toward preventive, alternative and holistic approaches to health. In the current system, researchers don’t have enough incentive to study generic drugs and root-cause therapies that look at things like diet.
I note once again that the NIH already has a fairly well-funded center to examine these questions, the National Center for Complementary and Integrative Health (NCCIH), formerly the National Center for Complementary and Alternative Medicine (NCCAM). Of course, research into the “preventative, alternative, and holistic approaches to health” funded by NCCIH includes rank quackery such as acupuncture and highly dubious treatments like chelation therapy for cardiovascular disease. This proposal sounds as though RFK Jr. wants to expand NCCIH to take up half of the NIH budget, which would, of course, be a disaster for public health. I also note once again that one of the most efficacious and safe preventative approaches to health is vaccines. I’d love it if the NIH put more resources into vaccine research, but somehow I suspect that RFK Jr. isn’t including vaccines in the category above.
In fact, in a recent interview:
View on Threads
View on Threads
View on Threads
I have been trying to locate the full version of this video in order to find the context (even though just this 24 second clip is bad enough), thus far without success. Apparently it was some sort of Tik Tok townhall done earlier this year, before RFK Jr. suspended his campaign:
I also note that RFK Jr. didn’t mention cancer in this video clip, which is rather why I want the whole video to examine. Finally, “functional medicine” quack Dr. Mark Hyman is in on this discussion, because of course he is. In any case, in the video RFK Jr says:
I’m going to go to NIH my first week, and I’m going to call all the division heads and I’m going to call all the division chiefs, and I’m going to say: We’re going to give drug development and infectious disease a break, a little break, a little bit of a break, for about eight years, and we’re going to study chronic disease.
This is an incredibly stupid and dangerous idea. For one thing, it’s a false dichotomy. Some infectious diseases are chronic diseases or produce chronic diseases. Hepatitis B and C come to mind, which can both result in chronic liver failure. For another thing, infectious diseases don’t care about your ideology. During that eight year “pause,” we could face another pandemic. The overall budget for the National Institute of Allergy and Infectious Diseases (and allergies are also chronic diseases) is just over $6.5 billion, out of a $47 billion total NIH budget. It’s minuscule in the scheme of things. Moreover, we are increasingly approaching a crisis due to bacteria resistant to our most powerful antibiotics, with the World Health Organization declaring that antimicrobial resistance (AMR) is “one of the top global public health and development threats. It is estimated that bacterial AMR was directly responsible for 1.27 million global deaths in 2019 and contributed to 4.95 million deaths (1).”
Moreover, the NIH already does fund research into chronic diseases. Here are the budgets for the last five years:
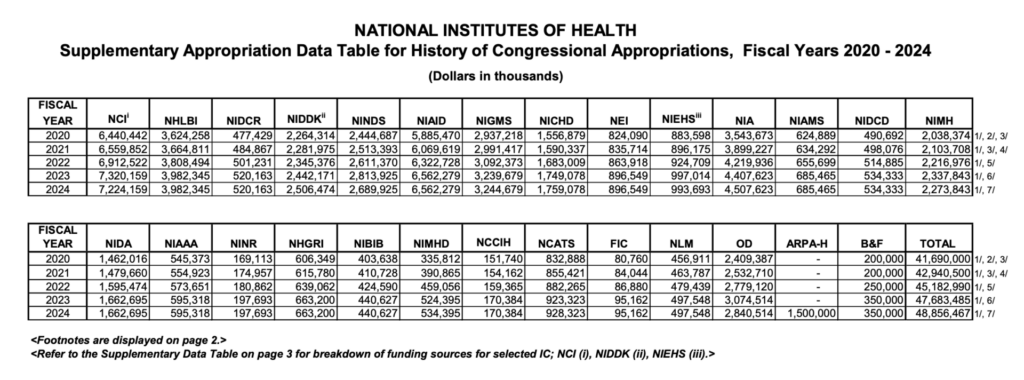
Look at how much goes to National Heart, Lung, and Blood Institute, to study heart and lung diseases, most of which are chronic. Ditto the National Institute of Diabetes and Digestive and Kidney diseases, the National Institute of Mental Health, and the National Cancer Institute. (Cancer is now a chronic disease for many people, and the HPV vaccine, for example, can prevent cervical cancer.)
Those of you who have been reading SBM for a while know that what RFK Jr. is really referring to when he talks about researching “chronic disease” is researching diet, exercise, and all sorts of woo as the be-all and end-all of preventing and curing such diseases. What he’s really advocating is that we should “pause” drug development and infectious disease research in favor of research of the sort carried out by the National Center for Complementary and Integrative Health (NCCIH).
Enter Dr. Jay Bhattacharya
I realize that Dr. Jonathan Howard just wrote about how Dr. Jay Bhattacharya, whose role in promoting the Great Barrington Declaration and, more recently spreading pandemic misinformation and fear mongering about COVID-19 vaccines, has floated to the top of the list of potential candidates for NIH Director. Previously, speculation had been that he was a top candidate for the post of CDC Director.
Bhattacharya, who holds a medical degree and PhD from Stanford, has never held a senior government position, nor any role overseeing a large bureaucratic organization. While that might have stymied his candidacy in prior administrations, Kennedy and his allies view his inexperience as a positive, saying they are seeking reformers willing to battle the bureaucracy.
Yes, putting someone who’s never run a large organization before in charge of a large organization always ends well. In any event, putting Bhattacharya in charge of the CDC or NIH would be bad, with the potential to damage public health for a generation, and I’m still not quite sure which would be worse. Whichever is worse, it looks like a fair bet now that he will be nominated for NIH to replace Francis Collins, and to that end he has been furiously sucking up to RFK Jr. in posts like RFK Jr Will Disrupt the US Medical Establishment. If you want to see how far Bhattacharya’s nose is up RFK Jr.’s rectum (far enough to be able to see his uvula from the inside), try not to gag or laugh too hard as you watch Bhattacharya swallow what’s left of his scientific pride in order to dismiss RFK Jr.’s 20 year history of bonkers quackery, antivax conspiracy mongering and pseudoscience, and just plain wrongness:
Left-leaning outlets, such as the Atlantic, Washington Post, PolitiFact, and Forbes— as well as the predominantly Left-leaning medical establishment — were quick to lambast the choice, using selective quotations and a narrow focus to smear Kennedy. But establishment mandarins who focus on his sometimes eccentric scientific claims, from vaccines to AIDS, overlook the single most important factor in his success: the anti-science, authoritarian policies of the Covid years. As a result, they miss what matters most in the Kennedy phenomenon: his broadly appealing, and thoroughly centrist, reform agenda.
And:
The central argument against Kennedy from the medical establishment pertains to some of his scientific claims, for example about vaccines, wireless radiation and cancer, raw milk, and neurodevelopmental disorders caused by water fluoridation. Kennedy is not a scientist, but his good-faith calls for better research and more debate are echoed by many Americans. If he remains true to this promise, scientists will be able to work to address the challenges of evidence in ways that previous administrations have not. The status quo is not working for the public interest or patients. If the medical establishment becomes obsessed with resistance, it will marginalise itself and lose what little trust the public currently places in it.
Translation: Never mind all the dangerous antivax quackery RFK Jr. has promoted, you know, his “sometimes eccentric claims” that were “selectively” quoted. Never mind his 20 year history of promulgating conspiracy theories about cellphone radiation and cancer, water fluoridation, and raw milk. Don’t worry about them! Forget about it! After all, RFK Jr. isn’t a scientist; so it’s all good. He can be taught. (No, he can’t. We’ve been trying to teach him for two decades, and he only gets worse and worse.) To this, I would add something that Bhattacharya must surely know but can’t admit: RFK Jr.’s calls for “better research” are not in good faith. He has already said that there are no vaccines that he considers safe and effective and that basically nothing can change his mind. His standard of evidence is very much a double standard. He demands impossible standards of evidence for what he fears (vaccines, pharma drugs) but accepts what he likes (“functional medicine,” and quackery for chronic disease) based on flimsy to nonexistent evidence.
But what would Bhattacharya do? According to this news article:
Bhattacharya has long called for changes to NIH and other government agencies in critiques that began before the pandemic. In a 2018 working paper, Bhattacharya and co-author Mikko Packalen, an economist at the University of Waterloo, wrote that NIH could “do more to promote innovative science,” arguing that scientific and political considerations may have led the agency to inadequately fund exploration into new ideas. Two years later, Bhattacharya and Packalen concluded in another working paper that scientific breakthroughs had stagnated because scientists were wrongly focused on being cited by other researchers.
The devil, of course, is in the details. Many are the brave maverick scientists who have castigated NIH for being “too conservative” in deciding who gets funded. I’ve discussed this issue a number of times, most recently when Bhattachary’s Stanford colleague John Ioannidis (who’s also a Great Barrington Declaration believer) complained about the NIH supposedly promoting “mediocrity” and “conformity.” His arguments were, as is often the case, exaggerated. First, most of the time, the examples cited of science that led to innovative treatments whose investigators initially had difficulty getting NIH funding are often exaggerated and full of hindsight bias, in which now it seems obvious how brilliant the ideas were but at the time they were being considered it wasn’t at all obvious. I will note, as I always do, that whenever NIH funding decisions become more conservative, it is usually be cause money is tight and study sections and advisory councils don’t want to make risky bets. The answer to that is to provide more funding. Does anyone want to take a guess whether Donald Trump will significantly increase NIH funding? More likely it will be quite the opposite.
One frightening thing about Bhattacharya is that he mistakes the criticism that he justly received for being “silenced” and wants revenge. Indeed, in 2022, he wrote about how he wanted to hold “lockdowners” accountable:
He made allusions to the Civil War, envisioning himself on the victorious side:
I observed at the time that Dr. Bhattacharya’s frequent invocation of the “laptop class” as COVID-19 bogeymen unconcerned about the harms their interventions were causing always struck me as a combination of a straw man so enormous that if set on fire it could be seen from space plus breathtaking hypocrisy. After all, no public health official advocating business closures and shelter-in-place orders early in the pandemic denied potential harms. (It’s not their fault that governments didn’t adequately support those whose livelihoods were impacted by such orders.) Moreover, Dr. Bhattacharya himself is most definitely part of the “laptop class.” Although he is an MD, he’s a Stanford University academic and researcher, not a clinician. He never did a residency and, as far as I can tell, never practiced clinical medicine after medical school, which means that he has never treated a COVID-19 patient, nor has he struggled (for example) to provide care to cancer patients (as I have), due to the effects of the pandemic overwhelming hospitals and, now, due to severe staffing shortages now affecting my hospitals and many others. He could easily do most of his work from home, and I’d be willing to bet that in 2020 and through much of 2021 he did.
Yet, having been ensconced in his ivory tower and home office, in October 2020 he joined his fellow GBD authors Martin Kulldorff (then a professor at Harvard) and Sunetra Gupta (a professor at Oxford) at the headquarters of the libertarian “free market” think tank American Institute for Economic Research (AIER) for a confab with like-minded AIER officials, reporters, and scientists to discuss a “natural herd immunity” approach to the pandemic, ending “lockdowns,” and using “focused protection” for the elderly and those at high risk of severe disease and death from COVID-19. The result was the GBD, which advocated a “natural herd immunity” approach to the pandemic, ending “lockdowns,” and using “focused protection” for the elderly and those at high risk of severe disease and death from COVID-19.
Also, as Dr. Howard mentioned just yesterday, Bhattacharya has spend the last four years portraying himself as the “canceled” outsider, whom The Man crushed for his “scientific heresy” and how he has spent the past four years portraying himself as a total outsider, even though he had advised presidents and governors and become a “dissident” scientific rockstar among the right doing so. Given what he’s written, I suspect that, although Bhattacharya might share RFK Jr.’s “eccentric” beliefs with respect to COVID-19, masking, public health, and COVID-19 vaccines, he fears being associated with RFK Jr.’s utterly reality-divorced views with respect to vaccines in general, his conspiracy theories, and all the quackery that he supports. I also suspect that he thinks that, as a “reasonable” scientist, he can rein RFK Jr. in from his more bonkers beliefs and do what he wants to do with the NIH without all the collateral damage that would come from RFK Jr. getting his way.
How well did that work out with Donald Trump? Not very, and I predict that it won’t work out either for Jay Bhattcharya or any of the other contrarian doctors who tried to downplay just how conspiracist, pseudoscientific, and full of quackery RFK Jr.’s views on health are. He will become complicit in damaging or destroying the greatest engine of biomedical research and discovery in the world, the NIH.